Why wouldn't a fellow endoscopist sent their patients for a procedure that is as effective, safer, with no significant recovery time, and far less expensive when compared to surgery?

Dr. Gandolfo is a board-certified gastroenterologist in Long Island, NY. He is the founder of Retroflexions.com and enjoys writing about healthy living and the practice of medicine. He started his solo practice, Precision Digestive Care, in 2018.
Why wouldn't a fellow endoscopist sent their patients for a procedure that is as effective, safer, with no significant recovery time, and far less expensive when compared to surgery?

The question of cost is a valid one, especially at the current time where health care costs seem to be spiraling out of control. Many times it seems that the outcomes gained from large health care expenditures do not justify the massive costs, or are not feasible to implement for society as a whole.
MILAN, Italy: Gastroenterologists rejoice! Innuendo Technologies has announced that FDA approval of the di Michelangelo robot is expected early this spring...the first robotic platform designed specifically to perform fecal disimpaction! Dr. Hans Enyuanus was one of the pioneers of robotic fecal disimpaction using the di Michelangelo® System, having performed over 2000 procedures...

I read with interest your blog today, and then some of your other offerings. I am a rural general surgeon who has done 12,000 colonoscopies in 35 years. My question is how do we know that screening is effective at reducing mortality?

There is a lot going on this month: colon cancer awareness events, flexing for $$$, new and old blog posts, and a birthday!

The phrases "mind-blowing" and "fecal transplant study" are not often used in the same sentence (or even in the same publication), however when I read the following study about fecal transplants, my mind was in fact blown!
No self-respecting gastroenterologist would use premade stool, just like no self-respecting Italian would use jarred sauce, right?

It was only a matter of time that a fecal transplant product was created. Now instead of having to test an individual donor and mix the stool to prepare the specimen for delivery through the scope, one can simply call the hospital pharmacy several hours before the fecal transplant is scheduled and order a 250 mL bottle of frozen donor stool from OpenBiome.

After taking a few months off, I've totally revamped the site with a clean and modern look and I am very excited to start writing again! However, it's not just the aesthetics of the site that are changing. Over the past year or so, I have seen a dramatic increase in the traffic to the site

Over two years ago, I had a colon resection for the removal of a cancerous tumor (stage 2A). Ever since, I have had on and off bleeding in my stool. My surgeon has done two sigmoidoscopies and my gastro doctor has done two colonoscopies.
What is immediately apparent from these numbers is that Cologuard rarely misses cancer. However, if we count polyps as a significant finding, there are plenty of false-positive results (45%) and plenty of false-negatives too (34%). So is Cologuard a good test overall?
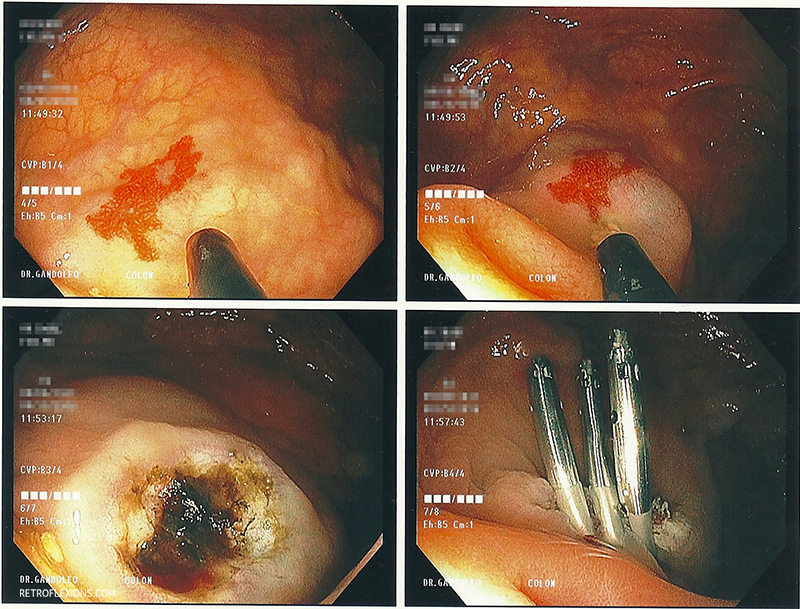
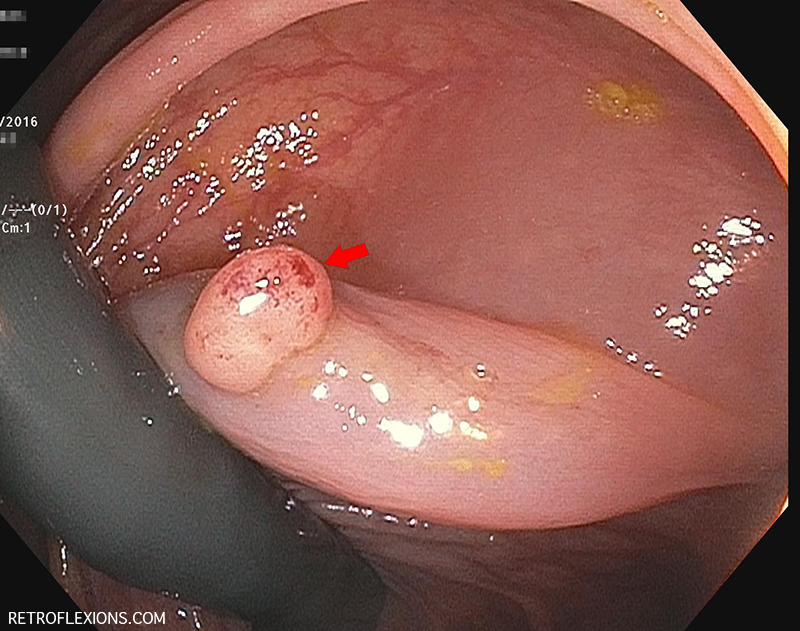
One useful technique to minimize the risk of perforation when treating large angiodysplastic lesions (let's arbitrarily define large as greater than 10-mm in diameter) is to...

When someone has a real disease and tells me they're not a pill person, I can't help but wonder what exactly does that mean? Someone with dangerously high blood pressure, who is not a pill person will soon become a stroke person.
Should retroflexion in the right colon become a routine part of screening colonoscopy? Let's frame this question with the following facts: Colonoscopy is less-protective against right-sided cancers (which implies that colonoscopy is less-effective at finding or removing right-sided polyps...
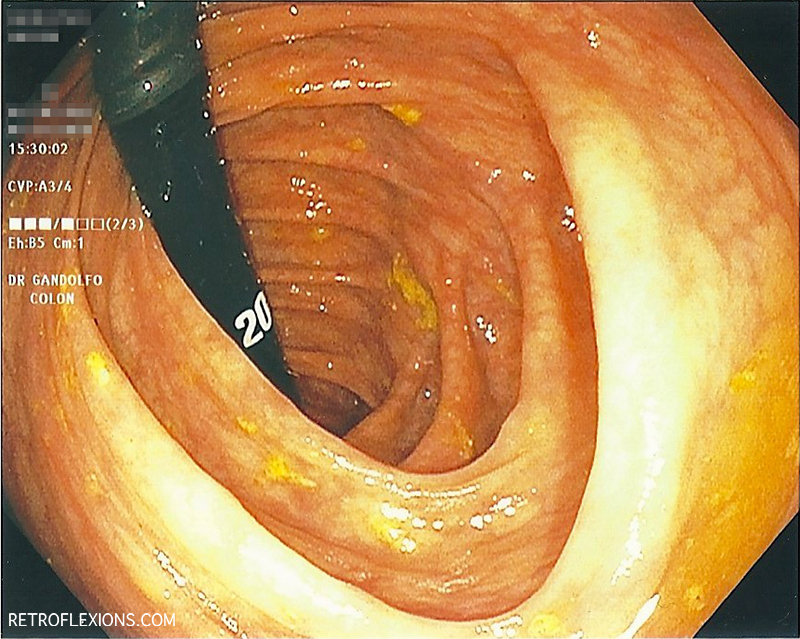
Since the name of my site is Retroflexions, it's about time I wrote an article about how to retroflex! More specifically, how does one retroflex in the right colon? (Fair warning: This article is probably only interesting to gastroenterologists.)
Make sure to never miss a post by subscribing!