
Remember early March 2020? Things were pretty normal back then. We were beginning to hear more and more about this new coronavirus thing, but had no idea what was about to happen in the weeks to come. My biggest concern surrounding my practice was that it was growing rapidly and I needed to figure out a good way to keep delivering personalized care to my patients. I was thinking about how to best expand the practice, and had some big plans for this year. I was very optimistic and looked forward to what the year would bring…
Man Plans and God Laughs
Then all of a sudden, COVID-19 was here in our faces, and life as we knew it had changed forever. Social gatherings were banned. Schools were closed indefinitely. Work was done from home–or not at all, as millions of able-bodied people were ejected from the workforce while businesses closed by the thousands. The economy grinded to a halt. And then there were all the poor patients who were infected with coronavirus along with the rising death tolls. Medical personnel on the front lines are facing shortages of personal protective equipment (PPE) like masks and faceshields, and patients are facing critical shortages of vital medical equipment like ventilators and many medications.
A few weeks prior to this nightmare it was business as usual in the outpatient gastroenterology world. If a patient came in (physically!) to see me in the office I was able to speak with him or her face-to-face without the fear of contracting (or passing on to them) a potentially deadly virus with a long asymptomatic incubation period. If my patient needed a procedure, we would book the procedure and I would do it! Sadly, as I write this, the simple idea of seeing patients and scheduling endoscopic procedures is no longer possible.
Everything changed. Within the span of a few days, all of the major medical societies came out with statements regarding how to prepare for the tsunami of COVID-19 patients that was coming our way in only a few weeks time: Stop all elective care, stop routine procedures, stop face-to-face visits in offices, and clear out the hospitals as much as possible! We needed to make room for all of the patients who would be coming, just as they had come in China, then Italy, Iran, Spain, and South Korea. We needed to free up nurses and doctors to take care of these patients. We needed to conserve PPE and repurpose operating rooms and recovery areas for patient care. These areas would have to function as intensive care units in the weeks and months to come…
Adapt and Overcome
Now what? How can I continue to take care of my existing patients and keep the practice alive? And what about people who develop new non-COVID-19 gastrointestinal issues during this pandemic? How will they get care if all the doctor’s offices are closed?
Let’s not forget that without seeing patients or performing procedures, I won’t be able to keep the doors of my practice open forever. There is a lot of overhead to cover when running a medical practice, from the usual stuff like rent, utilities, and payroll, to the more medically-specific fees like the absurdly high malpractice insurance premiums and expensive electronic medical record (EMR) programs that we are forced to use.
Well I guess I could just close the practice and go to work for a hospital, or just leave medicine entirely and do something else. But I struggled and worked for years to get this practice to the place it was in early March 2020, and I don’t want all of that hard work and sacrifice to go to waste! Furthermore, I have training and skills in this field that took over a decade to obtain, and these skills are much-needed right now…it would be foolish to throw it all away and run. But how can I be a doctor if I can’t see patients in my office?
Enter Telemedicine!
Telemedicine refers to real-time audio/video communication between a doctor or other healthcare provider and a patient. It’s basically like having a Facetime call or a Zoom meeting with your doctor from the comfort of your couch at home.
As soon as the coronavirus pandemic started ramping up in the United States, telemedicine went from a non-covered service to something that insurance companies and Medicare all of a sudden provided coverage for! But not many doctors were ready to just jump in and start seeing patients using telemedicine: During the second week of March, within only a 48-hour time frame, most of us went from “business as usual” to “The world is on fire, cancel all patients and lock the front doors of the office” after hearing escalating warnings and mandates from multiple health authorities.
The reason for our lack of preparedness regarding telemedicine was not because this is a new or complicated technology…in fact it has been around for many years! However, insurance companies have been slow to adopt this method of patient care, and vastly prefer that you (the insured patient) waste hours of your precious time by: 1) driving to your doctor’s office; 2) sitting around and filling out redundant paper forms; 3) waiting to get seen by the doctor; and 4) driving back home. Medical care was like this because “that’s the way it’s always been” or some other inane argument. We have been told for years that telemedicine is not something that is covered by insurance, only to be told overnight that telemedicine is going the be the only way to see patients for the foreseeable future…so of course no doctor was prepared for this paradigm shift!
Furthermore, there were a lot of questions about telemedicine to answer without any real notice or guidance:
- What kind of hardware will a doctor and patient need to have a telemedicine visit? (I cover this below.)
- How do you take care of a patient without physically seeing him or her in the office? This may work great for some specialties, but would be difficult for others. For example, you can’t have a prostate exam using telemedicine!
- How are doctors supposed to code and bill these visits to make sure they are getting reimbursed appropriately from the patient’s insurance company? It’s not like the doctor wanted to close his or her practice for the next few months. Are the insurance companies actually going to cover these services when the smoke clears? Will there be a thousand little rules and conditions that ultimately lead to denials until the doctor figures out the nuances of what each and every plan wants?
- What are the legal ramifications of treating patients using telemedicine? Are we more likely to miss something serious because we are not physically touching the patient? Are doctor’s opening themselves up to malpractice based on limitations imposed by this viral pandemic and the need to comply with physical distancing recommendations?
So what is a doctor to do when their physical well-being is threatened by a deadly virus, and their practice is threatened with financial catastrophe at the same time? Well, when patients get COVID-19, many of them need to go on life support using a ventilator. When a small business is not able to function due to external circumstances beyond anyone’s control, it will either die or need a life support system too. In the case of my small practice, part of that life support system is the small webcam I bought two weeks ago. (And just like that ventilator, due to high demand, these little webcams are in short-supply and difficult to find too!)
Here is how telemedicine works from the point-of-view of a patient:
- You call the office for an appointment.
- You are given an appointment time and we email you some paperwork to do on your device.
- Instead of driving to the office, parking, filling out forms in the waiting room, etc., you simply find a spot in your house where the WiFi signal is good and keep your phone or tablet handy (a computer works too).
- You get an email or text invitation when the doctor is ready to start the appointment. Just click the link!
- The doctor and patient speak together during a real-time video encounter and formulate a treatment and follow-up plan.
- The doctor sends any necessary prescriptions or test orders to the patient electronically.
- Bonus: Neither party gets COVID-19 during the encounter!
How I Set Up My Office for Telemedicine
This is probably only relevant for healthcare providers looking to set themselves up to do telemedicine, so if that’s not you, feel free to skip this section!
This is how I did it…keep in mind there are probably twenty different ways to do this, so this is just one person’s opinion.
The gear
First you need some type of camera. I got a webcam (Logitech C920s but any webcam will do) which I think is the best solution because the image quality is good and there is a microphone built in. It was easy to install, just plug-and-play. It was hard to find, as all online sites seemed sold-out, and I had to search all over Long Island to find one in a random Staples store 30 minutes away…but I got it! That being said, you can also use a laptop since most have webcams built-in, or a tablet or even a smartphone, although it is much easier and looks more professional to just have a dedicated webcam.
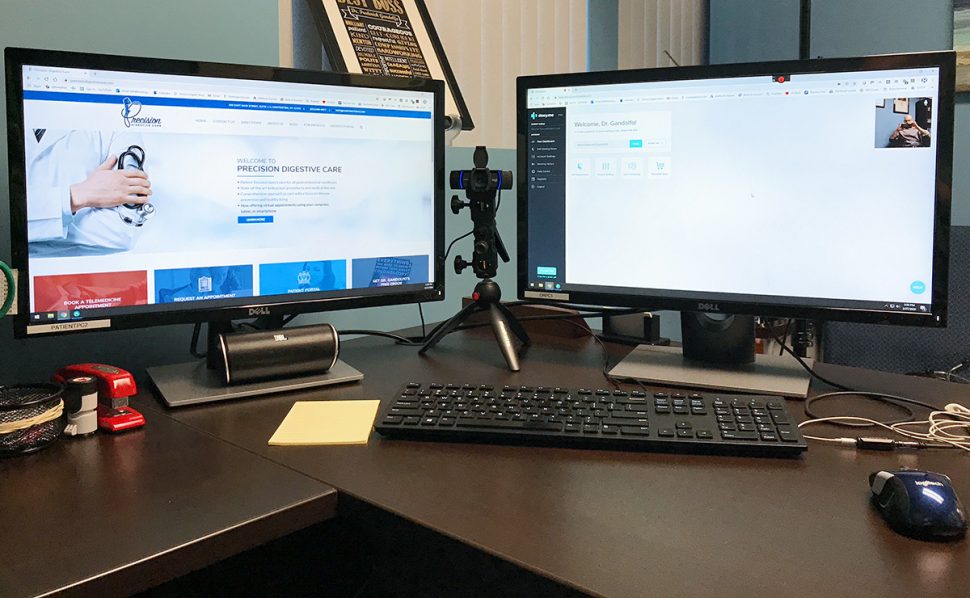
A second computer monitor is optional but highly recommended if you plan on seeing more than a handful of patients per week using telemedicine. This allows you to keep one monitor dedicated to the telemedicine platform (this is where you will see your patient) and the other monitor can be used to access the EMR. This prevents the need to open and close windows to try to cram everything into one screen. Monitors are relatively cheap, but just make sure that your computer can accept dual monitors, and that you have the correct cord to hook the second monitor up. I needed a special cord called a DisplayPort to HDMI cable, which I discovered after the fact.
I also have a small tripod and umbrella adapter to hold the camera at the right height between the monitors. I happened to have this stuff around, being a camera nerd and wannabe YouTube sensation, but you can get them pretty easily online. I like having the camera at eye-height rather than on top of the monitor so I look more natural for patients, and they are not forced to stare at the top of my bald head.
Also, make sure you have a pair of headphones or earbuds. I am just using the ones that came with my iPhone, but almost anything will do. This helps a ton by cutting out feedback which can lead to annoying echos.
The software
There are a ton of telemedicine platforms out there! You can choose one that integrates with you EMR and office scheduling software, and has a ton of fancy features, or you can choose a simple stand-alone platform and figure out a way to work this with your EMR. You also need to figure out if you want your patients to have to download an app and create an account to use your platform, or if you simply want them to open a browser window on nearly any device and log in using a more simple process.
I am a simple guy, so I was more comfortable with a simple solution. I wanted a stand-alone platform that had all the basic functions I needed (like being able to send text and email invites when you are ready to start the visit) and most importantly did not require my patients to set up an account or download anything. They simply click the link I send them via text or email right before the encounter, or they can just go to the website and login with their name to show up in my “virtual waiting room.” Simple is good. Complicated processes lead to failure and frustration, and simply put–I don’t want to have to deal with people not being able to download or install apps etc. It’s just too much of a headache.
I chose to do telemedicine using a service called doxy.me. So far it has been great! I am using the “professional plan” since the free plan really does not have the functionality that I need. The best part is the setup: You can set up your account and start seeing patients on their platform in only a few minutes. Other services can have lengthy on-boarding processes…who has time for that?
The logistics
Here is the headache part: How do we efficiently treat patients that never set foot in our office? What about the basic history? Do we need to review their medication lists, allergies, home address and emergency contact number, insurance information, pharmacy address and primary care doctor’s phone number at the time of the visit? Of course not! But how can we effectively collect this information, which is usually done on paper at the time of the first visit while the patient is in the waiting room? What about all of those legal and financial forms that need to be signed, such as HIPAA, assignment of benefits, office policies, medical records releases, and so forth? How do we collect a copay?
Again, there are probably ten different ways of doing this, but this is what I settled on: I made all of my office forms into “fillable” PDF forms. The demographic forms are filled out digitally by the patients, and the forms that require signatures are sent using Adobe Sign software. Patients are also paying copays and deductibles using credit cards. This whole process takes a few emails and phone calls, but what other choice is there?
Anyway, that’s it. Just get a device with a camera, pick a platform to use, create some financial policies and if you’re computer savvy you can make all your forms electronic like I did…it’s a simple project if you know how to use Adobe Acrobat. If you’re not computer savvy, just hire someone who is able to help you.
The whole goal for me was to create an automated process that my staff can do without any input from me. I want to be able to simply sit down and see telemedicine visits and take care of the medical stuff. If that requires a few emails and credit cards to be used, so be it. This system needs to run efficiently, so that I can devote the rest of my time to helping with the onslaught of COVID-19 patients that are hurtling towards our local hospital as I write this…
What does the future hold?
No one knows! The absolute disaster that is COVID-19 will unfortunately take countless lives and bring the world to its knees for at least the next several months…and likely longer. I will be seeing patients using telemedicine for now, until it is safe to have real face-to-face visits in the office again. And once adequate PPE is available to purchase again, I will have a lower threshold to invite patients into the office on a case-by-case basis. After all, not every gastroenterology-related illness can be handled using telemedicine, and we can’t forget about all of the patients with non-coronavirus related problems that left untreated are equally or even more dangerous that COVID-19!
For now, my immediate future is going to be split between working shifts at my local hospital to help treat all of the coronavirus patients, and seeing GI patients a few days per week using telemedicine. It will be a strange dichotomy between seeing sick high-acuity COVID-19 patients which also carries a higher personal risk of exposure, and seeing the lower acuity and zero-risk telemedicine patients. Interesting times indeed.
What about the future of telemedicine? Once life goes back to “normal” (which will unfortunately be a new normal, and likely not the carefree times of 2019 when we didn’t have to worry about shaking a person’s hand), I expect that telemedicine will be here to stay in one way or another. Patients will realize that their physical presence is not always needed for medical care to happen. This will create less strain on the entire medical system, from patients who no longer need to take a half-day from work just to see their doctor for a routine matter, to doctors who won’t need to crowd their waiting rooms with people, to the highways and parking lots of our towns.
Telemedicine will also release patients from the geographic limitations regarding who they can see for medical care. If you, as a patient, find a doctor in your state that you really like, but that doctor is located 2 hours away from your house, you can perhaps make a pilgrimage to the office once and then continue follow up via telemedicine. Even if insurance stops covering this valuable service, I will bet that there will still be a demand due to the convenience factor: Two hours of my time during the weekday is worth way more than the few bucks that I would have to pay out-of-pocket for a telemedicine appointment!
Closing thoughts
Nothing is guaranteed. Our future, both near and far, is quite uncertain and things are changing hour-by-hour. We can complain about this and feel sorry for ourselves, or we can accept that this is now our current reality. If we are still healthy, we can count our blessings that we have not been affected by the virus yet, when so many others have already died or are still fighting a painful fight. As a business-owner and independent doctor, I can wallow in self-pity while I watch the practice that I worked so hard to build slowly crumble because patients cannot come in for appointments and I cannot perform procedures, or I can do whatever I can with telemedicine and be happy that I still have a job when so many others have been laid off through no fault of their own. As a physician, I could hide at home, paralyzed with fear of getting the disease, or I can realize that I actually have the training and experience to truly help people during this unprecedented time of need, put on a mask, and jump into the fray.

How Can I Book a Telemedicine Appointment?
Visit the practice website for more information at https://precisiondigestivecare.com/telemedicine/
Daphna Mitchell
March 30, 2020 at 11:39 PM
UMmmm very interesting, Dr. Gandolfo. My therapist and I are using doxy and it works. What about my ophthalmologist – my glaucoma (I do drops 5 times a day) and cataracts; my gastroenterologist – I’ve had major surgery in my poor tummy and I’m 78 and losing weight. Etc. etc. etc. I’m a retired biglaw attorney and know how to work from home with all the right toys … but how do you actually diagnose and treat by webcam??? We’re losing touch??? instruments??
Thank you for everything you do and care about.
Frederick Gandolfo, MD
March 31, 2020 at 4:59 AM
Thanks for the comment. It’s not the optimal solution for every specialty, but for right now it’s the best thing we have! I would hazard a guess that 85% of GI patients that I see can be seen via telemedicine without needing a physical exam. Even the ones that do need an exam, this can sometimes be deferred for a while while we first do some lab testing, stool testing, imaging, trial of medication, etc. It’s really only the acute abdominal pain that should be physically seen. The history provides 90% of the diagnosis.
Charles W
March 31, 2020 at 1:59 PM
Do you think that a general shift toward telemedicine will result in less professional satisfaction for physicians? No doubt that taking good care of patients counts most toward professional satisfaction, which is the good part of telemedicine in times like this (and perhaps other situations you mention, where an office visit isn’t necessary but a follow-up is). But I’ve been fortunate to personally like the doctors I have seen over the years, and I think they like seeing me too. From the aspects of your personality I can glean from your columns and videos, I’m sure you also like seeing your patients. To the extent that personal interaction contributes to professional satisfaction, it must be diminished by video visits. I use video all the time in my job (lawyer), but it’s just not the same as visiting with my clients in person, even if we can get the same work done.
Frederick Gandolfo, MD
March 31, 2020 at 2:47 PM
This is a great comment. I think that for now, professional satisfaction will come from being able to provide much-needed patient care…so yes, telemedicine is leading to professional satisfaction. Once the crisis is over, I am sure we will go back to seeing patients face-to-face (can’t wait for that actually!), but I think telemedicine will have a niche for patients that live far away, are not mobile, are too frail to come it, or who prefer it due to not having to take time off work etc to see a doctor.