Coffee is enjoyed all over the world, perhaps more than any other substance except for water and air. We all are familiar with the stimulant effects of coffee, and independent of this effect caffeine is also a weak mood-elevating substance. There are many social rituals that revolve around coffee too. In fact, this blog probably would not exist if it wasn’t for strong black coffee (I would be sleeping instead of writing!)
However, did you know that coffee is good for your liver? There are numerous studies that show some correlation between a healthy liver coffee intake. Researchers are not entirely sure if it is coffee as a whole (which is composed of many different substances) or caffeine itself (the stimulant substance in coffee) that has the beneficial effect. What does seem to be clear, is that people at risk for chronic liver disease who drink coffee (studies have shown as little as one cup per day) seem to develop less fatty liver disease, less cirrhosis, less liver cancer, and are less likely to die as a result of chronic liver disease!
The hepatic stellate cell is the mediator of liver fibrosis (scarring) and eventually cirrhosis. When activated by various insults to the liver (e.g., alcohol, chronic hepatitis, etc.), the stellate cell starts laying down proteins that promote scar tissue formation. One theory on how coffee improves liver disease is that caffeine inactivates these stellate cells, thereby slowing the process of cirrhosis.
We must be cautious to not put too much weight in these studies however. Mostly, they are retrospective cohort studies, and therefore rely on self-reporting of coffee intake. The self-reporting bias is well known and can skew the results dramatically. Also, retrospective studies can only demonstrate correlation, not causation. It’s one thing to say “coffee drinkers often have less liver disease.” It’s another thing entirely to say, “drinking coffee prevents liver damage.”
Black coffee is the best!
As a gastroenterologist, I often tell people to limit coffee intake for various reasons. For example, coffee can contribute to acid reflux. In some people, coffee can overstimulate the GI tract and cause diarrhea. Too much caffeine can cause anxiety, poor sleep, or heart arrhythmias. Drinking a $5+ coffee drink from Starbucks with cream and sugar may also negate any health benefit of coffee since the extra calories and fat probably do more damage in the long run, not to mention the detrimental effect on your bank account. However, if we are just focusing on the liver, I can tell you to drink that coffee up!
If you enjoyed this article, sign up for our free newsletter and never miss a post!
References:
Khalaf N, White D, Kanwal F, et al. Coffee and caffeine are associated with decreased risk of advanced hepatic fibrosis among patients with hepatitis C. Clin Gastroenterol Hepatol 2015;14:S1542-3565.
Morisco F, Lembo V, Mazzone G, et al. Coffee and liver health. J Clin Gastroenterol 2014;48:S87-90.
Setiawan VW, Wilkens LR, Lu SC, et al. Association of coffee intake with reduced incidence of liver cancer and death from chronic liver disease in the US multiethnic cohort. Gastroenterology 2015;148:118-25.
Wang Q, Dai X, Yang W, et al. Caffeine protects against alcohol-induced liver fibrosis by dampening the cAMP/PKA/CREB pathway in rat hepatic stellate cells. Int Immunopharmacol 2015;25:340-52.
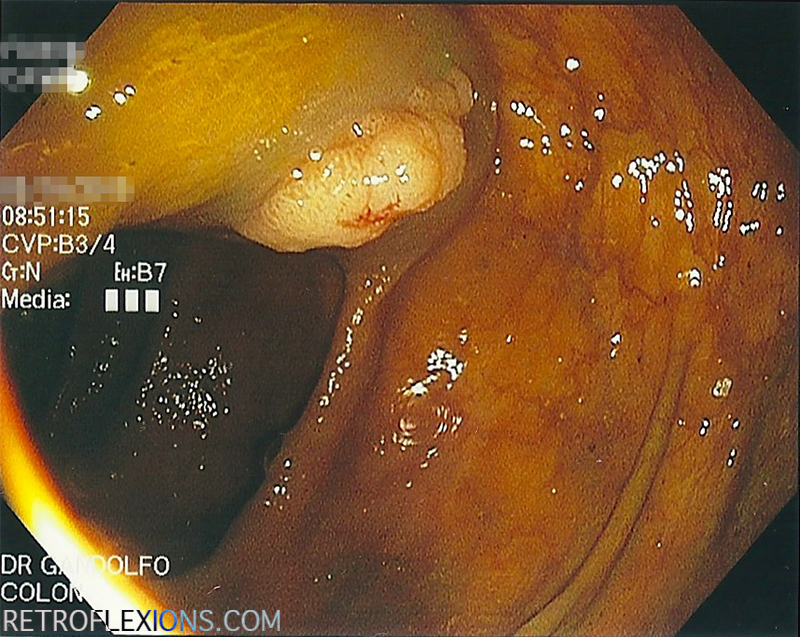
Removing polyps is the only way to prevent colon cancer before it starts. That is the entire point of a screening colonoscopy. Precancerous colon polyps (adenomas) are found in a large number of patients and there are usually no symptoms whatsoever. Polyps don’t cause pain. There is usually no significant bleeding, or at least not the kind of bleeding that a patient can see (the exception being large polyps in patients on blood thinners.)
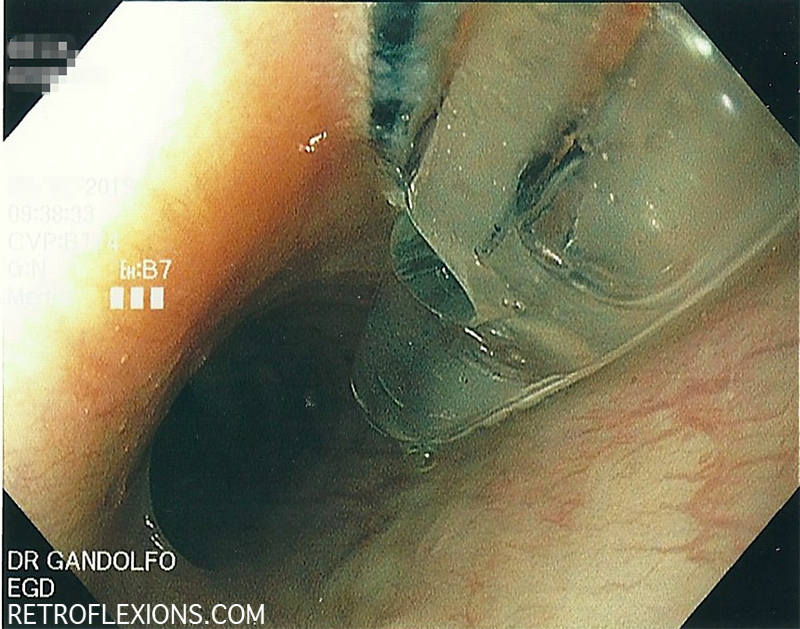
Villous adenoma found in the ascending colon on routine screening colonoscopy.
There is excellent data showing that the better the endoscopist is at finding adenomas during colonoscopy, the better protected the patient is from later developing colon cancer. Doctors that find more precancerous polyps and then remove them are simply providing better patient care. If a polyp is there hiding out in the colon, and missed on colonoscopy, then the protective effect of the procedure on reducing the development of colon cancer in the future is lost.
The adenoma detection rate (ADR) is currently the best “report card” for colonoscopy performance available. To figure out the ADR, simply count up the number of screening colonoscopies done over some time period, and also figure out how many patients in that group had at least one adenoma found. Divide the two numbers (patients with adenomas found/total procedures performed) and that is the adenoma detection rate (multiply by 100 to get the percent.) So for example, if I performed 100 screening colonoscopies over some time period, and 42 patients out of that 100 had at least one adenoma, my ADR would be 42%.
The benchmark for adenoma detection rate was formerly suggested at 20%. However, with more and more data coming out showing that the true prevalence of adenomatous polyps is much higher, it seems that 20% is setting the bar too low. This year, a task force of all the large governing bodies in gastroenterology published new quality guidelines and (not surprisingly) the ADR was raised to ≥25% on average (men ≥30%, women ≥20%). In my opinion, the ADR is the single most important number that can be used to describe the quality of an endoscopist’s performance in colonoscopy. In fact, for each one percent increase in ADR, there is a three percent decrease in the development of colon cancer in the future!
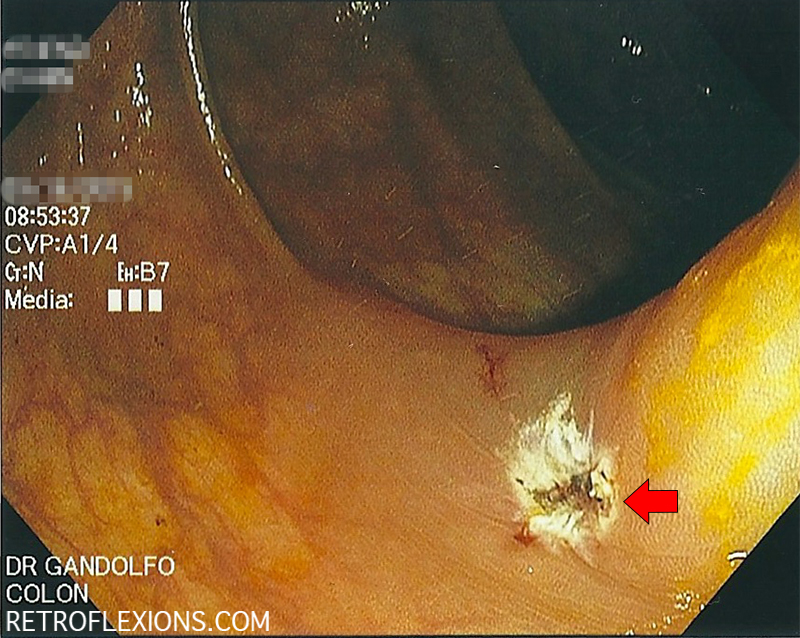
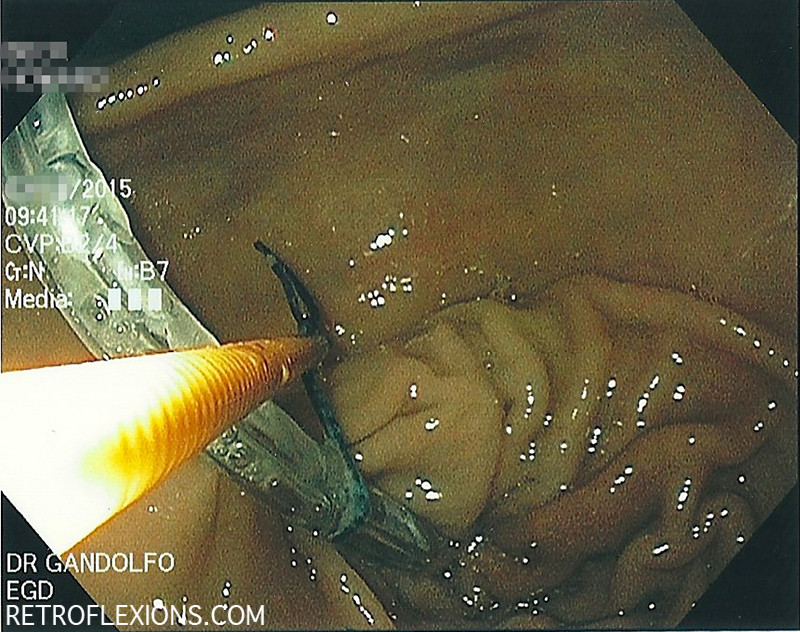
The polyp was injected with saline to make a cushion underneath to allow safer resection (white arrow shows the edge of the cushion).
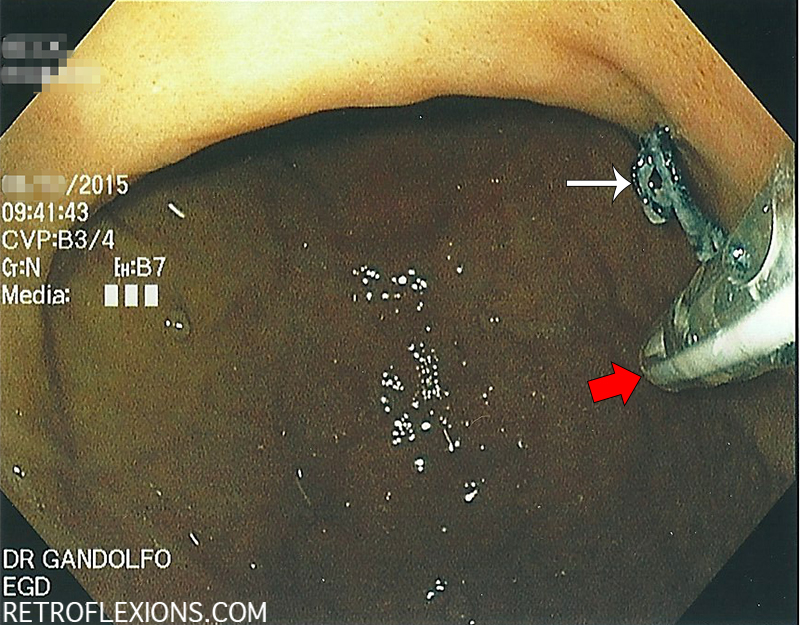
After resection with snare electrocautery, the base of the polyp (red arrow) is free of any remaining tissue. This is considered a complete resection. The polyp is then retrieved and sent for testing.
As the concept of standardizing quality and using quality metrics (such as ADR) evolves and becomes more commonplace, I would bet that patients and referring physicians will start to pay attention to what these numbers mean. All doctors that perform colonoscopy are not equally good at it. All endoscopists should be measuring their own individual ADR, and working to push that number higher and higher.
And for patients, don’t be afraid to ask your doctor what his or her ADR is. Not everyone currently measures their ADR, so don’t be totally alarmed if they’re not exactly sure. They should at least know what the bare minimum is supposed to be (≥25%.) Just hope you don’t get a confused look like “what’s an ADR?”
If you enjoyed this article, sign up for our free newsletter and never miss a post!
Reference:
Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Am J Gastroenterol 2015;110:72-90.
Filed under: Gastroenterology and Endoscopy
Comments: Comments Off on What is the “adenoma detection rate” and why should I care?
As a patient, you only have control over a few parts of your colonoscopy. Usually you have a choice of which doctor does the procedure. You have a choice of showing up on the day of the procedure vs. running in the other direction. And finally, you have control on how well you are “prepped” for the procedure.
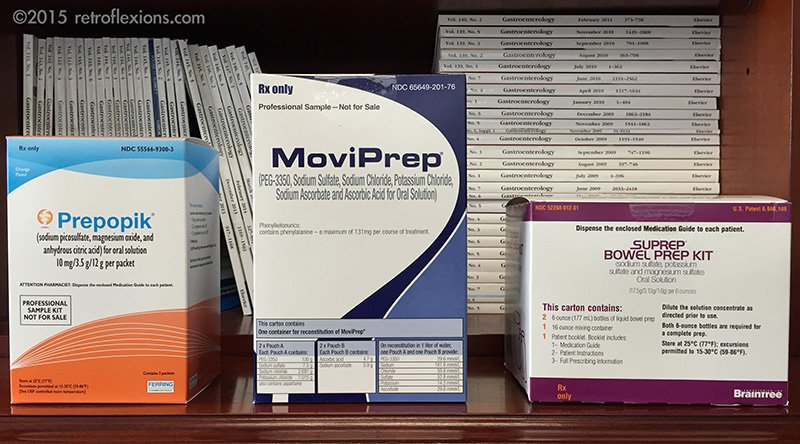
Various bowel preps that are optimized for split-dosing.
Bowel preparation (“prep” for short) is the most important patient-controlled part of the colonoscopy. Done properly, the inside of the colon looks as clean as the inside of a mouth. Ideally, after taking the prep, there is no stool or residue left behind, and the endoscopist can get a good view of everything. If there are polyps or other issues present, a good prep allows the doctor to see and address these findings. The procedure is usually shorter because less time is wasted trying to washing out the colon while you are under anesthesia. The procedure is safer because the doctor can see better. You are usually more comfortable at the end of the test because the doctor didn’t have to pump in as much gas during prolonged efforts to clean out the remaining debris in the colon.
The opposite of a good prep is a poor prep. In a poor prep, either thick liquid stool and particles, or solid stool are still present in the colon. This cannot just be flushed away during the exam, and therefore there will usually be one of two outcomes: the procedure will be aborted due to not being able to see anything meaningful; or the next colonoscopy will be recommended at an earlier date (e.g., in less than six months). Either way, you (the patient) are exposed to all the inconveniences of a colonoscopy (the day off work, the anesthesia, the risks, the cost, etc.) and none of the benefits (preventing colon cancer, or finding what was causing bleeding/symptoms, etc.)
There are several ways to maximize your chances of successfully completing the bowel prep. In no particular order, here they are:
Follow the printed instructions from the doctors office regarding the prep and diet to follow before your colonoscopy. Read this a few days before the procedure, not after lunch the day before the procedure!
Make sure you have all required prep materials in the house: the actual prep from the pharmacy, any over-the-counter stuff you need (e.g., dulcolax, magnesium citrate), and any clear liquids you may need.
Plan ahead and refrigerate the prep if possible to make it easier to drink.
Tell your doctor if you have had a problem with the prep in the past, there may be another alternative prep or schedule you can use.
Split-dose bowel prep is both easier to tolerate, and gives a better prep. If your doctor hasn’t prescribed the prep this way, ask him or her why not.
Don’t think that since you are having diarrhea after only finishing half of the prep, that the second half is optional…it’s not! The second half is actually more important than the first and needs to be completed. This is the part that really washes out all the “debris” that sticks to the walls of the colon.
The prep can make some people nauseated, and vomiting can be common if you try to drink the prep too rapidly. If you are feeling full or nauseous, just slow down. Give yourself a break for a half-hour and try again. Don’t be a hero and try to “chug” the prep as fast as possible and then end up vomiting up the whole thing!
If you have questions or issues regarding the prep, don’t be afraid to call the doctor’s office the day or night before the procedure. I would rather you call than have a poor prep and have to then repeat the colonoscopy!
Remember that the goal of a screening colonoscopy is to prevent colon cancer, so give yourself the best chance possible by doing a good job with the prep!
Update 9/2019: I made a video that will help you get through your bowel prep! Check it out below!
If you enjoyed this article, sign up for our free newsletter and never miss a post!
Bad news is always hard to break. I would like to think that I get better at breaking bad news after doing it over and over, but it doesn’t make it easier. Some experiences stick with you and this is one of them:
Several years ago I was making rounds in the hospital and my next patient was an almost ninety year old man who was admitted several days earlier with progressive weight loss and abdominal pain. A CT scan done on admission showed a large mass in the pancreas with innumerable metastases in the liver–an incurable disease. A biopsy of one of the lesions was already done two days earlier, and we were waiting for results. In the meantime, the patient was not eating or drinking well, and was basically bed bound. This is what is called a “poor functional status” meaning that the patient is already quite debilitated from his advanced disease and will likely do poorly with aggressive treatment such as chemotherapy.
Just before seeing the patient, who I had never met before, I discovered that the biopsy results just came back and confirmed what all the other doctors suspected. Adenocarcinoma is what the report read (bad results are always printed in bold.) I introduced myself and began talking to the patient, who was alone and still unaware of the formal diagnosis. He seemed up-to-date on what was happening to him, and knew that he had “spots” throughout his liver and pancreas. “Did those results come back yet?” he asked. I told him that the biopsy results just came in this morning, and asked him if he wanted them now. He said “yes, tell me.”
After a long explanation which basically boiled down to the word “cancer” and after staying to answer his new questions and concerns, I called his primary doctor to relay the news. “Did you tell him?” the primary doctor asked, almost accusingly.
“Of course I told him…he wanted to know,” I said. I was confused why she asked me that way, and a little put-off that she thought I was going to shirk my painful responsibility of being the first to break the bad news. Wasn’t it his right to know what was going on with his body? Besides, I thought to myself, wasn’t it somewhat obvious by looking at the scan that we were dealing with something bad? Even if we took the word cancer out of the equation, an elderly man losing weight with months of abdominal pain and something growing where it isn’t supposed to is usually a bad sign.
In my head I wondered how she explained the recommendation to do a biopsy to the patient in the first place? Did she tell him what the possibilities were? I know that I always mention that we may find something “bad” if I am sending a patient for a biopsy and I expect to find something serious. Did she mention that the spots in the liver were metastases? Did she allude to the fact that once a cancer such as this is metastatic the goals of treatment no longer include the word “cure?”
Another phone call about 20 minutes later filled in all the blanks. It was the patient’s daughter calling me, distraught and irate. Still at home and preparing to come in to the hospital, she chastised me for “telling dad what he has! How dare you! Is this what they’re teaching in medical schools these days?” The patient’s daughter soon stated that she wanted to be the one to tell him the bad news herself. I tried to explain the situation, that I was unaware of these prior plans and that the patient had told me himself that he was ready for the news. In fact, I thought he took it quite well. At that time it didn’t matter anymore, the cat was out of the bag, and all I could do was apologize. I felt awful for adding this headache to her already very bad day. I am sorry I told your dad without you being there; I am sorry he has terminal cancer; I am sorry for causing you grief; I am sorry for everything.
Nowhere in the state-of-the-art electronic medical record was this most important fact found. No red box popped up making me click “acknowledge” that the patient is to be shielded from his diagnosis. Notes from his other doctors did not warn me. How could I have known? Even if I did know, is it right to hide the diagnosis from the patient, who is mentally competent and asking me to tell him? Is my duty to the patient or his family?
Perhaps it would have been best to do some reconnaissance first, asking the primary doctor, the nurse, and the patient who are the key players in the family, and who should be present for any serious conversations. The risk is that a white lie would need to be told to the patient who inevitably will ask “did you get the results yet?” before the family has arrived.
Let me go and check, I will let you know if they are back…
If you enjoyed this article, sign up for our free newsletter and never miss a post!
Nasogastric tubes (NGTs) are used to access the stomach either for drainage, or to provide access for feeding when a patient is unable to eat for various reasons. As the name implies, the tube enters the nose, and the tip sits in the stomach. Most of the time, the tubes can be easily passed “blindly” at the bedside without any special equipment or sedation. However, every once in a while, the tube cannot be passed for various reasons, often related to problems in the esophagus such as strictures, tumors, or large hiatal hernias.
Standard Salem Sump nasogastric tube and any available suture material (the needle was removed)
In these cases, blind passage of the tube is often impossible, and repeated attempts can be dangerous. Often endoscopy is needed to successfully place the tube into the stomach. This is usually a simple task, but can also become quite difficult since the tip of the NGT doesn’t always go where you want it to go. Also, getting the tube where you want it may be easy, however keeping it there while you remove the scope may be very hard because the friction between the tube and the scope drags the tube back out!
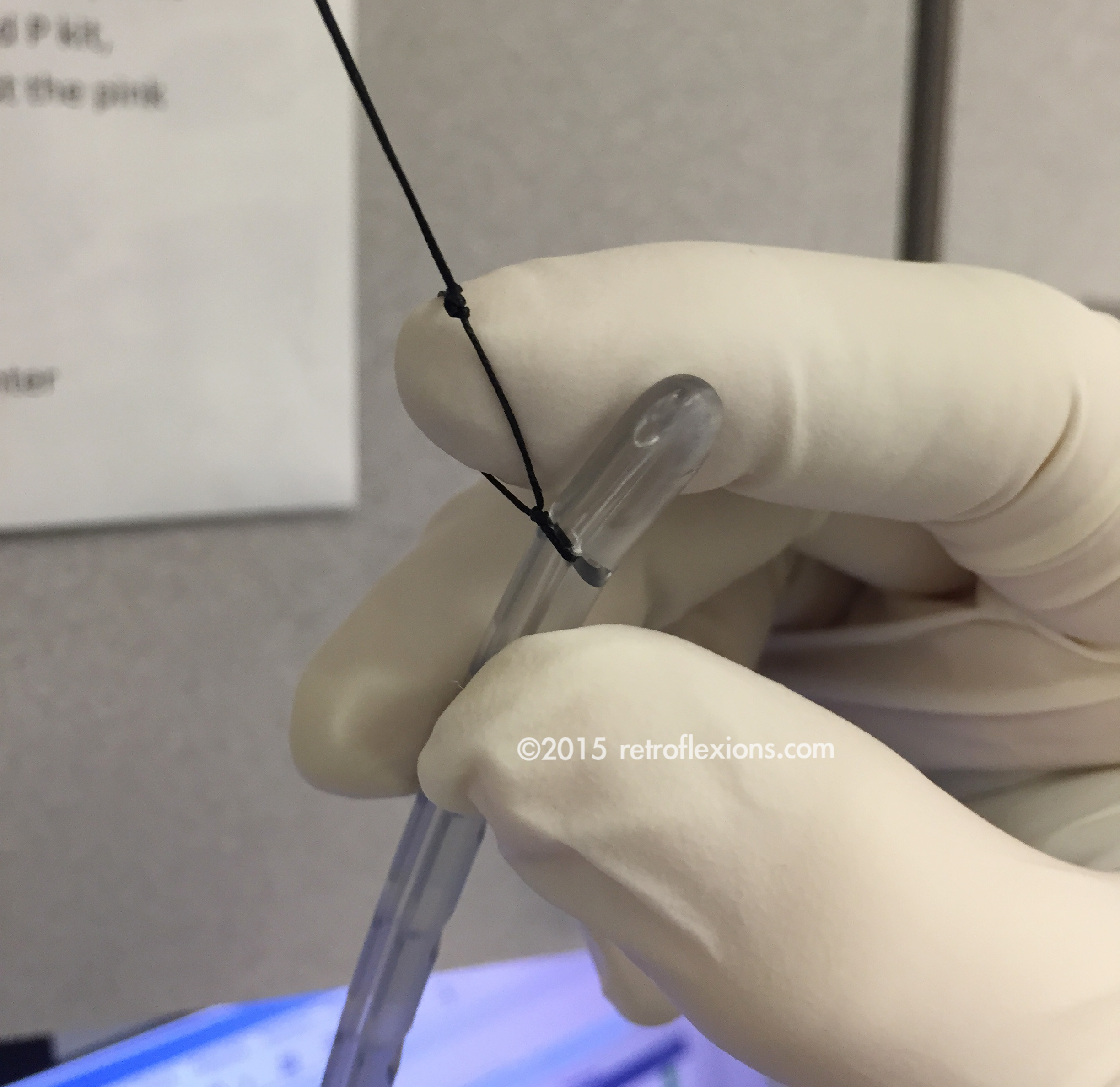
After tying the suture around the tip of the tube, form and tie a loop by using an assistant’s fingertip as shown above.
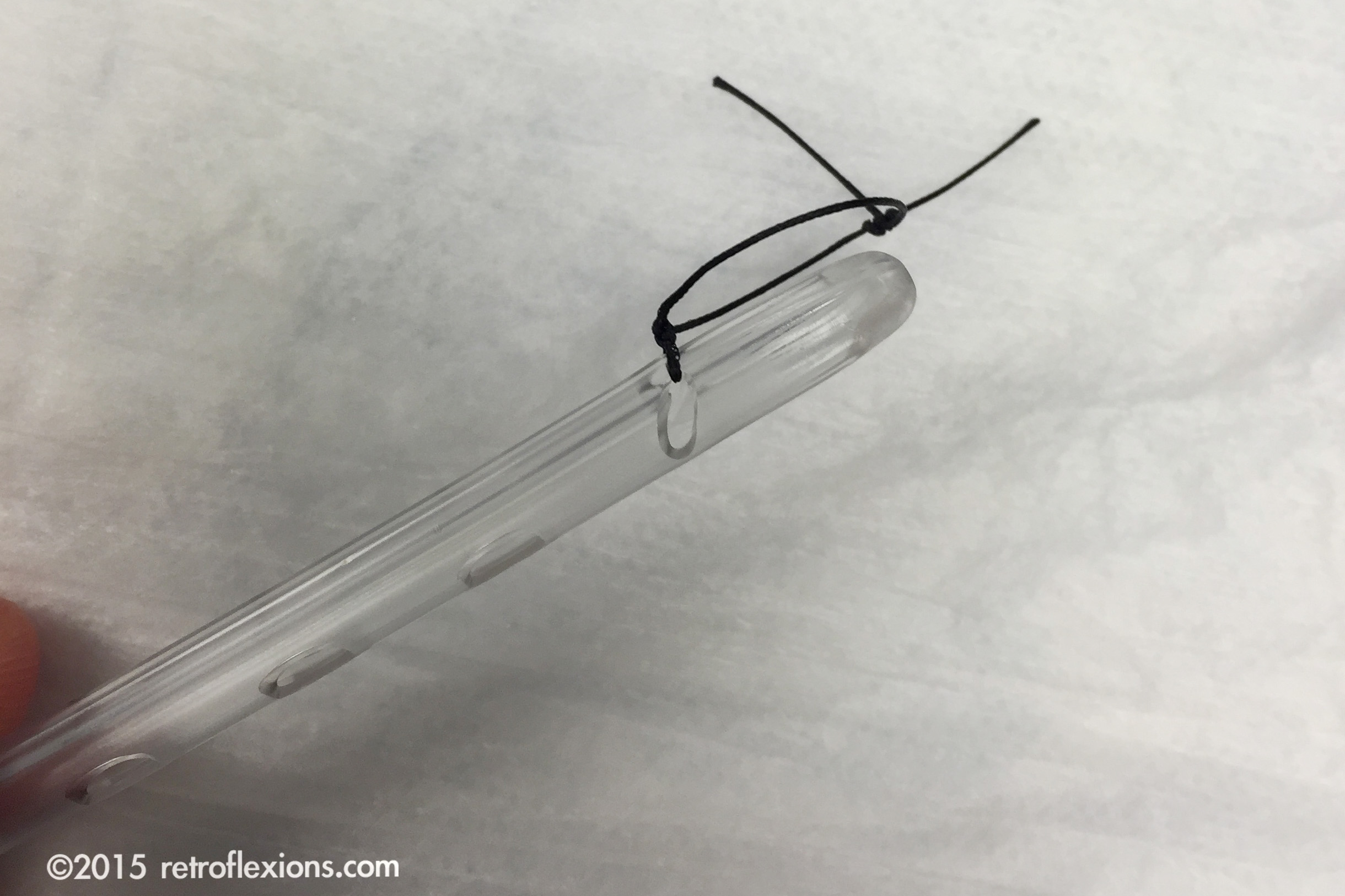
Here is the tube ready to be placed, with a small loop at the tip used to grasp and/or fix the tube once placed.
One technique that is helpful is to tie a suture (with a small loop in it) to the very end of the NGT. Once passed via the nose into the esophagus or pharynx, this suture can be used to grasp the tube with forceps and direct the tip wherever you need it to go. It also allows the application of clips to fix the tube in place (temporarily, in the case of a jejunal tube) in the small bowel which can prevent the tube from migrating out when you remove the scope. Sometimes I will even put a stiff guide wire through the lumen of the tube (using plenty of lube) to stabilize it while the scope is removed. Then the guide wire is removed afterwards. For an added margin of safety, if the tube placement was challenging I will usually check an X-ray afterwards to confirm the location of the tip before using the tube.
Tube with suture-loop in the esophagus. In this case, the patient had an esophageal ring that was preventing blind placement of the NGT.
A standard biopsy forceps (orange-colored instrument) is used to grasp the suture loop to drag the tube into the stomach.
Another picture of the tube placement showing the tube (red arrow) and the suture (white arrow). In this case, the tube was not fixed in place using clips.
Endoscopic tube placement is safe and effective when bedside placement is not possible. Other methods, such as radiologic tube placement are also effective, and the choice should be made based on local expertise.
If you enjoyed this article, sign up for our free newsletter and never miss a post!
Reference:
Gerritsen A, van der Poel MJ, de Rooij T, et al. Systematic review on bedside electromagnetic-guided, endoscopic, and fluoroscopic placement of nasoenteral feeding tubes. Gastrointest Endosc 2015;81:836-847.
Filed under: Gastroenterology and Endoscopy
Comments: Comments Off on Tips for endoscopic placement of nasogastric tubes
Nonselective beta-blockers (NSBBs) are often indicated for prevention of variceal bleeding in cirrhotic patients. However, there has been a large amount of data in the past several years that have raised serious concerns over the safety and utility of beta-blockers in patients with more advanced cirrhosis. Patients with what is considered decompensated advanced cirrhosis have now been shown in numerous studies to have increased mortality when treated with beta-blockers. Interestingly, most of the original trials on beta-blockers from the 1980s-era excluded these patients from study, therefore this important caveat was never recognized back then!
Beta-blockers blunt the sympathetic nervous system, which is a last-ditch survival mechanism to avoid systemic hypotension. Blocking this can lead to further decompensation in blood pressure and poor organ perfusion, especially of the kidneys. Hypotension, refractory ascites, and hepatorenal syndrome occurs, which is often the beginning of the death spiral of cirrhosis. In advanced decompensated cirrhosis, beta adrenergic tone is needed to survive, and blocking it is detrimental. To date, multiple high-quality studies have shown a dramatic increase in death among advanced patients who are treated with beta-blockers, with roughly a 20-45% absolute increase in mortality attributed to beta-blocker use. This is a huge effect!
Researchers have now been trying to define exactly when this advanced decompensated period occurs. There is still some debate in the area, but it is a pretty safe bet that the presence of diuretic-refractory ascites and/or the occurrence of spontaneous bacterial peritonitis (SBP) puts a patient into the advanced decompensated category. Here is a more comprehensive list of situations where beta-blockers are thought to be detrimental:
• refractory ascites
• systolic blood pressure < 100 mm Hg
• mean arterial pressure < 82 mm Hg
• acute kidney injury
• hepatorenal syndrome
• spontaneous bacterial peritonitis
• sepsis
• poor medical follow-up or poor compliance
In these patients, it has become my practice to stop any existing NSBB therapy (by slowly withdrawing the drugs over two weeks or so). In very decompensated patient with variceal bleeding, I would not start NSBB drugs for secondary prophylaxis either. Instead the focus should be on treating the variceal bleeding aggressively with endoscopic band ligation (tying off the varices with small rubber bands), or with placement of a TIPS (a shunt that reduces portal pressure dramatically). These data are practice-changing to me, and have broken a paradigm that has been in place in the literature for over thirty years.
If you enjoyed this article, sign up for our free newsletter and never miss a post!
The following are excellent references for further reading:
Ge PS, Runyon BA. The changing role of beta-blocker therapy in patients with cirrhosis. J Hepatol 2014;60:643-53.
Ge PS, Runyon BA. When should the beta-blocker window in cirrhosis close? Gastroenterology 2014;146:1597-9.
Mandorfer M, Bota S, Schwabl P, et al. Nonselective beta-blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology 2014;146:1680-90.