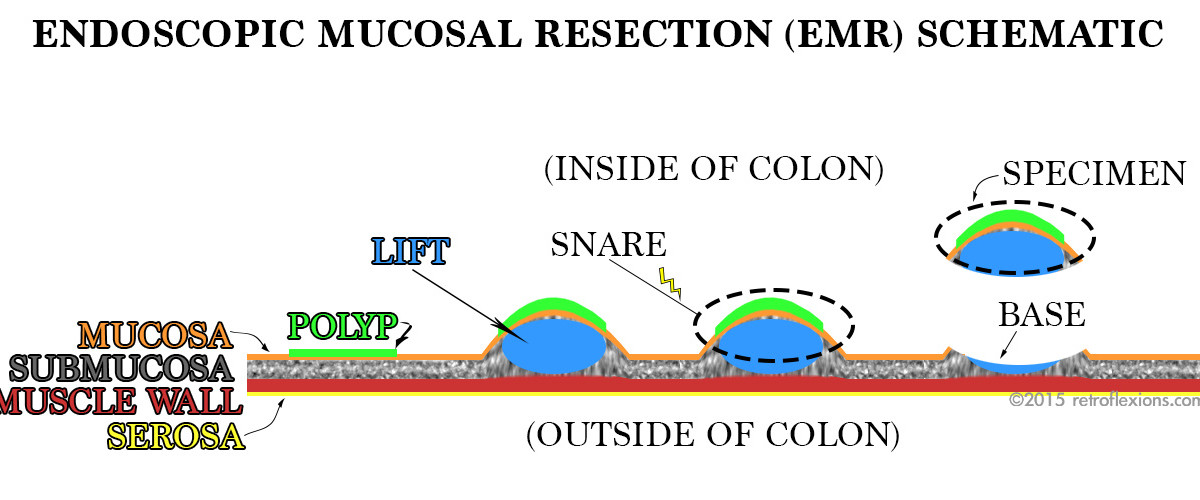
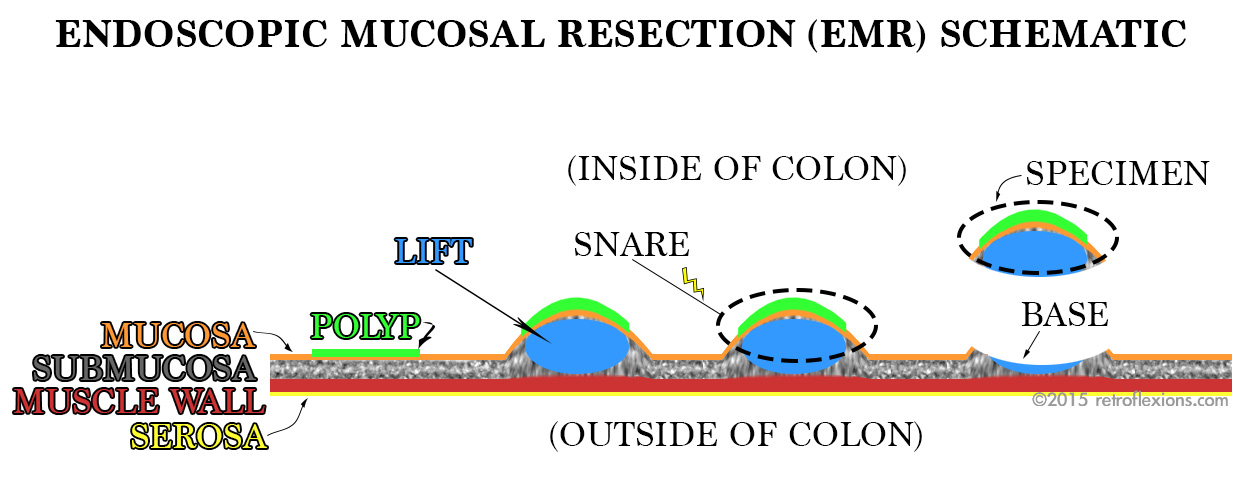
Simplified diagram of EMR of a flat colon polyp. The polyp (green) is lifted away from the colon wall (red and yellow) by injection of saline (blue) or some other substance into the submucosa (grey space). The lesion is then safely resected with snare electrocautery, without harming the muscle layer beneath.
Endoscopic mucosal resection (EMR) is a technique used to remove large polyps from the gastrointestinal tract. It works well for many different types of polyps, but is often reserved for large or flat polyps that cannot be removed by other endoscopic methods. Patients are often spared surgery for large polyps by having EMR done instead. Many lesions that have been deemed “not endoscopically resectable” can actually be safely removed by a gastroenterologist with training and experience in EMR.
Just as the name suggests, endoscopic mucosal resection is an endoscopic method of removing the inner layer of the GI tract (the mucosa). It is accomplished by creating a temporary space beneath the mucosa within the wall of the organ that allows the operator to safely work with much less risk of causing a complication such as perforation through the outer wall of the organ. Below the mucosa (the innermost layer), there is the submucosa. The submucosa is home to blood vessels and many supporting connective tissues for the organ.
By injecting fluid (usually saline) into the submucosa, this space is expanded much like inflating a balloon. With a deep submucosal cushion beneath, the mucosa can then safely be “shaved” off with a snare. In the case of a large polyp, this technique is repeated many times to resect the entire polyp in a piecemeal fashion.
There are many pointers and nuances of EMR, and these details will make excellent subjects for future articles. For now, I will just show a few pictures from a recent colonoscopy where the EMR technique was used to resect a large rectal polyp:
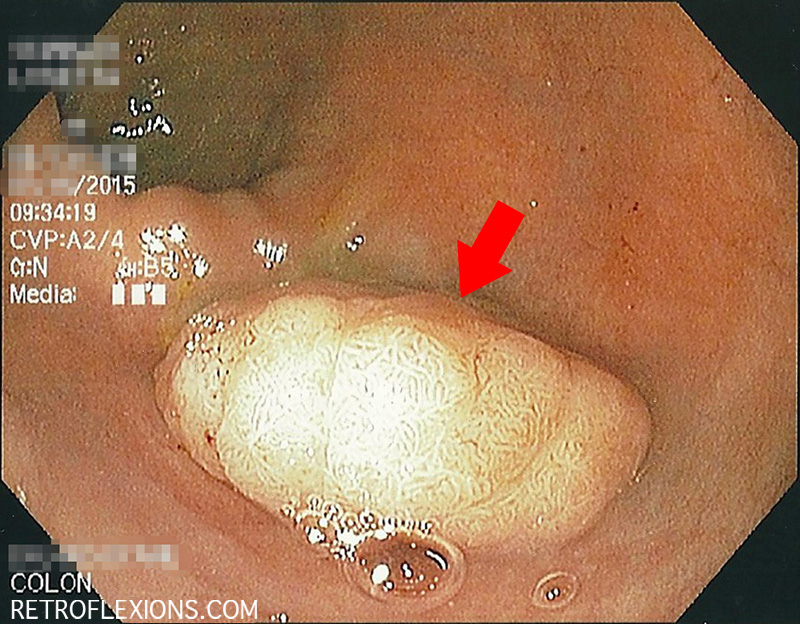
Sessile rectal polyp (red arrow) measuring approximately 2 cm across.

Retroflexed view after injection with saline and blue stain (methylene blue). Asterisk denotes area of submucosal lifting.
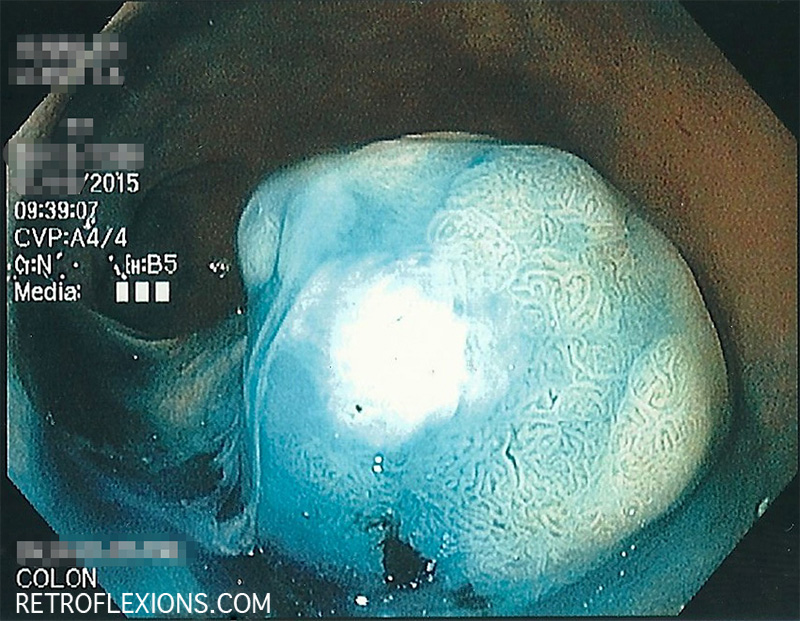
Some blue dye used to lift the polyp was sprayed on the surface. This can help to better identify the edges of the lesion by increasing contrast.

The resection base, after the polyp was removed with a snare. The white halo is cauterized tissue; the blue center is submucosa that was stained by methylene blue. This is considered a complete resection.
If you enjoyed this article, sign up for our free newsletter and never miss a post!