Case:
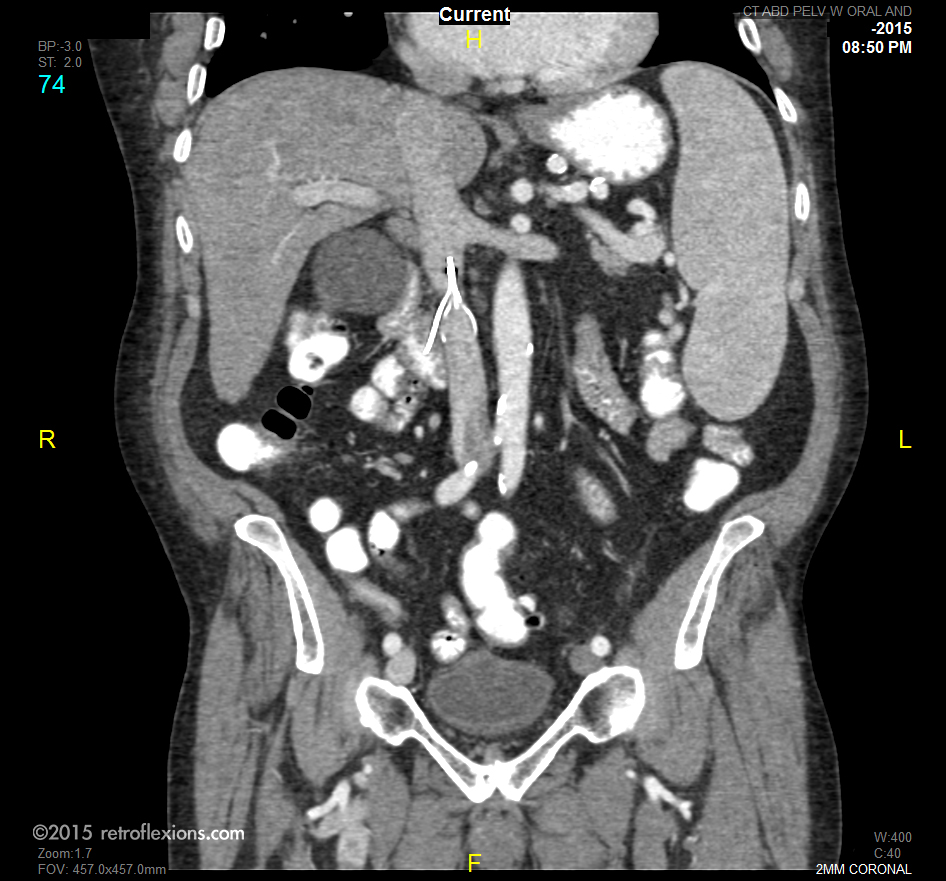
A 79-year-old man with a distant history of pulmonary embolism (PE) was admitted to the hospital with several days of vague right-sided lower abdominal pain. There was no history of gastrointestinal bleeding, and the pain did not worsen with eating. On physical exam, there was moderate right lower quadrant abdominal tenderness without rebound or guarding. Basic lab work was unrevealing. The patient underwent a computerized tomography (CT) scan of the abdomen, shown above.
The patient had a inferior vena cava (IVC) filter placed approximately seven years ago, after having a peri-operative PE. Here is the same scan, now with annotations:
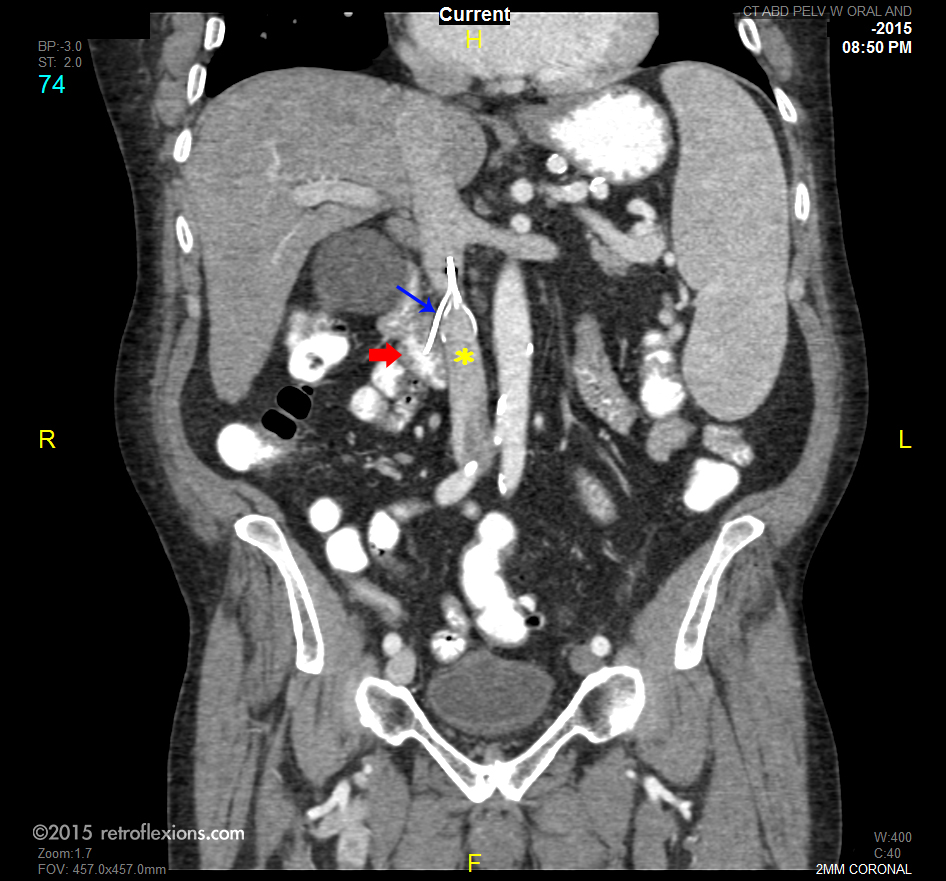
Red arrow: Duodenum (note the white oral contrast in the duodenal lumen). Blue arrow: IVC filter wire exiting IVC. Yellow asterisk: IVC.
Given the findings on CT scan, an upper endoscopy was performed to confirm the suspected duodenal perforation.
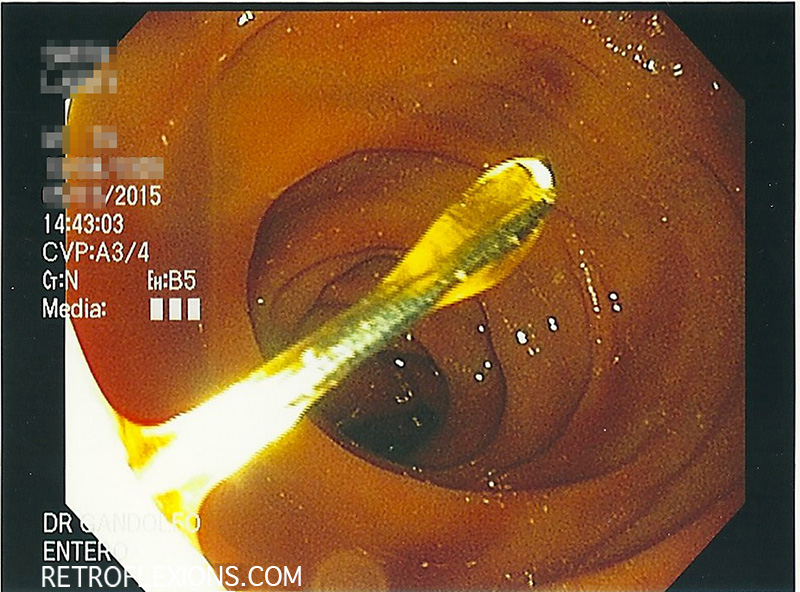
The metal prong from the IVC filter is clearly visible in the duodenum on endoscopy.
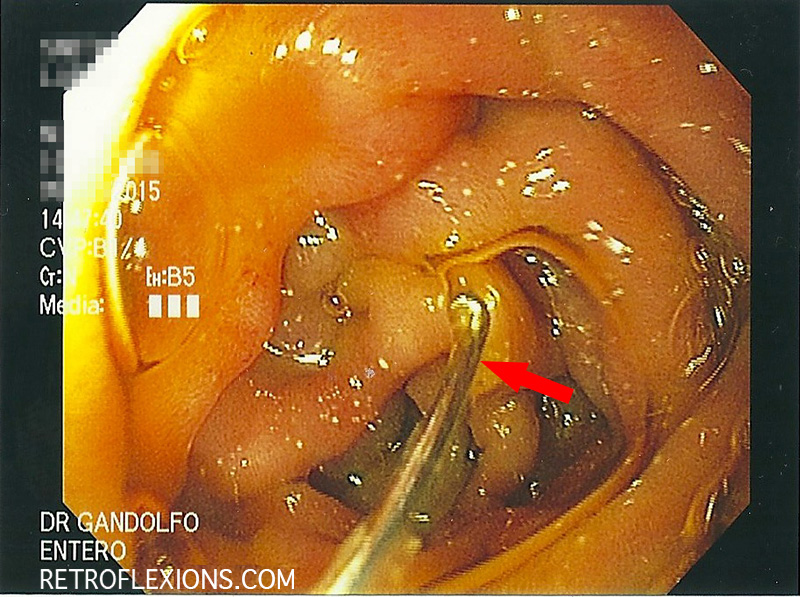
Another view showing the curved tip of the IVC filter prong (red arrow) in the duodenum.
Discussion:
IVC filters have been available since the 1970’s, and are typically indicated to prevent recurrent PE, or to prevent PE in patients that have contraindications to anticoagulation. Duodenal perforation by IVC filters is a rare event, and the true incidence is unknown. The reported incidence of any perforation of the IVC wall with filter placement is reported to be about 0.2% (2 patients out of 1000). The usual symptoms are upper abdominal pain, either epigastric or right upper quadrant, and/or GI bleeding.
In most of the published cases of duodenal perforation due to IVC filters, patients were treated with open surgical removal of the filter, with good results. In patients where the filter could not be safely removed due to an inflammatory reaction surrounding the filter, the prongs were trimmed flush with the wall of the IVC. Out of the twenty reported cases of operative intervention for perforating IVC filters, all patients survived and there was one thrombotic complication reported.
When reading studies of such rare events, it is important to remember the publication bias. That is, there is a tendency to publish successful cases, but usually unsuccessful cases or cases with bad outcomes are not published. Authors are simply afraid to attach their name to a complication publicly. Therefore, I am sure there are many more cases of duodenal perforation from IVC filters that have not been reported, just as I am sure there are cases where these filters were removed that had poor outcomes.
So what did we do with our patient? Since his pain was not in the typical location (his pain was in the lower abdomen), and since the patient was traveling from out of state, we chose to do nothing. The filter did not perforate the duodenum yesterday and may have been that way for years. There was no surrounding inflammatory reaction, and no GI bleeding. His pain resolved with watchful waiting and he returned home two days later. Long term, he may still need to have the filter removed to prevent complications down the road, or if the abdominal pain recurs.
If you enjoyed this article, sign up for our free newsletter and never miss a post!
Reference:
Malgor RD, Labropoulos N. A systematic review of symptomatic duodenal perforation by inferior vena cava filters. J Vasc Surg 2012;55:856-61.
Written informed consent was obtained from the patient prior to publication of this case report.